
Biomedical
Novel Liposomal Dry Powder Aerosol Inhalation
Novel treatment for pulmonary diseases
Airway mucus obstruction is a hallmark of various pulmonary diseases, such as asthma, chronic obstructive pulmonary disease (COPD), and cystic fibrosis (CF). Aerosol inhalation is commonly used in lieu of oral and intravenous antibiotics for chronic infection management. Dry powder inhalers (DPI) are an attractive form of aerosol inhalation for pulmonary drug delivery because they are propellant-free, intrinsically breath actuated, and have improved formulation stability. However, current DPI formulas are only able to deposit about 12-40% of the emitted drug dose to the lung.
The technology
Researchers at Virginia Commonwealth University have developed a novel liposomal dry powder inhalation formulation with superior respirable properties to enhance pulmonary drug delivery using excipient enhanced growth (EEG) strategy. The design is a highly translational muco-inert liposomal dry powder aerosol that is loaded with single or combined antibiotics to treat multidrug resistant germ-negative bacteria lung infections. This novel formulation is designed to be administered by handheld dry powder inhaler devices to improve patient compliance and treatment efficacy. It has been shown to rapidly diffuse in the airway mucous to reach the lung epithelium and achieve uniform airway distribution and prolonged lung retention, which is an improvement compared to conventional antibiotics-loaded liposomes that are shown to be restrained in mucus and get removed rapidly by the mucociliary and/or cough-driven clearance (Figure 1).
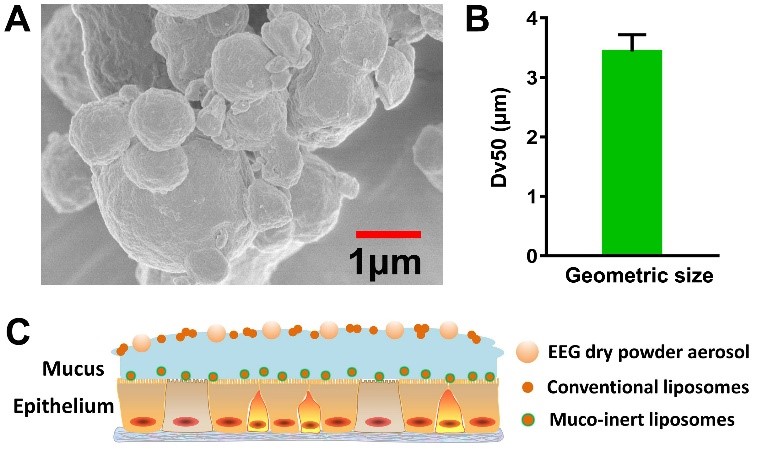
Figure 1. Respirable EEG dry powder aerosol formulation containing muco-inert liposomes. (A) morphology of EEG dry powder formulation containing muco-inert liposomes; (B) median geometric diameter (Dv50) of the dry powder aerosol formulation; (C) schematic of novel liposomal EEG dry powder aerosol delivery to the airway mucosal surface. Antibiotics loaded muco-inert liposomes could be released from the deposited aerosol particle and diffuse into the deep airway mucus, whereas the released conventional liposomes are trapped in the superficial mucus layer and finally be removed by mucociliary clearance and/or cough-driven clearance.